
The Ministry of Health and Family Welfare is a responsible for implementation of various health programmes on a national scale in the areas of health, prevention and control of major communicable diseases and promotion of traditional and indigenous systems of medicines.
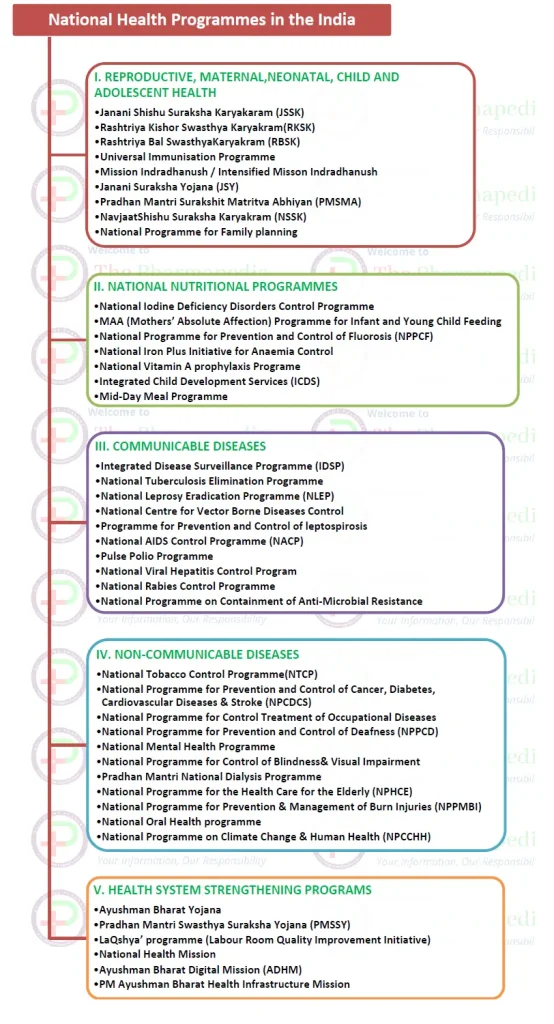
We are going to divide in 5 major classes the list of National health programmes in India.
- I- REPRODUCTIVE, MATERNAL,NEONATAL, CHILD AND ADOLESCENT HEALTH PROGRAMS
- II- NATIONAL NUTRITIONAL PROGRAMMES
- III- COMMUNICABLE DISEASES PROGRAMS
- IV- NON-COMMUNICABLE DISEASES PROGRAMS
- V- HEALTH SYSTEM STRENGTHENING PROGRAMS
I. REPRODUCTIVE, MATERNAL,NEONATAL, CHILD AND ADOLESCENT HEALTH PROGRAMS
These programs further can be categorized into following subclasses.
- Janani Shishu Suraksha Karyakaram (JSSK)
- Rashtriya Kishor Swasthya Karyakram(RKSK)
- Rashtriya Bal SwasthyaKaryakram (RBSK)
- Universal Immunisation Programme
- Mission Indradhanush / Intensified Misson Indradhanush
- Janani Suraksha Yojana (JSY)
- Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA)
- NavjaatShishu Suraksha Karyakram (NSSK)
- National Programme for Family planning
1. Janani Shishu Suraksha Karyakaram (JSSK)/ जननी शिशु सुरक्षा कार्यक्रम
- Government of India has launched Janani Shishu Suraksha Karyakaram (JSSK) on 1st June, 2011.
- The scheme is for pregnant women who access Government health facilities for their delivery.
- The following are the Free Entitlements for pregnant women:
- Free and cashless delivery
- Free C-Section
- Free drugs and consumables, transport, food/diet
- Free diagnostics
- Free diet during stay in the health institutions
- Free provision of blood
- Exemption from user charges
- Free transport from home to health institutions
- Free transport between facilities in case of referral
- Free drop back from Institutions to home after 48hrs stay
- The following are the Free Entitlements for Sick newborns till 30 days after birth. This has now been expanded to cover sick infants:
- Free treatment, Free drugs, Free diagnostics, Free provision of blood, free transport

2. Rashtriya Kishor Swasthya Karyakram(RKSK)
The Government of India on 7 January 2014 launched the nation’s first comprehensive adolescent health programme named Rashtriya Kishor Swasthya Karyakram (RKSK).
The RKSK defines an adolescent as a person within 10-19 years of age, in urban and rural areas, includes both girls and boys, married and unmarried, poor and affluent, whether they are in school or out of school.
To guide the implementation of this programme, MOHFW in collaboration with UNFPA has developed a National Adolescent Health Strategy. It realigns the existing clinic-based curative approach to focus on a more holistic model based on a continuum of care for adolescent health and developmental needs.
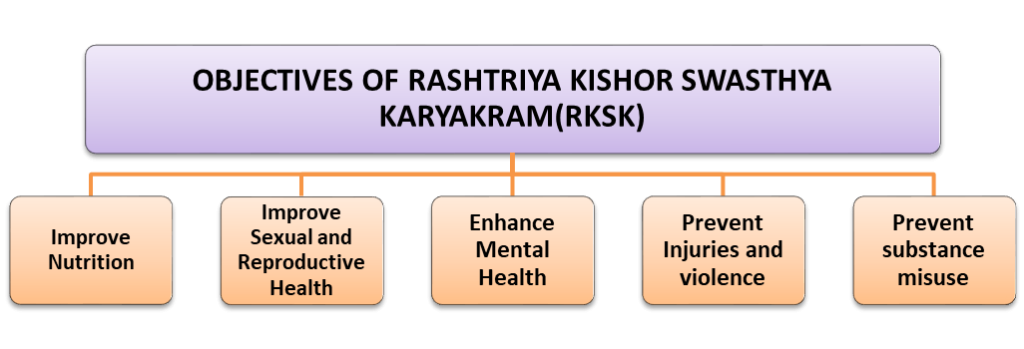
Objectives of the programme:
i. Improve Nutrition
- Reduce the prevalence of malnutrition among adolescent girls and boys (including overweight/obesity)
- Reduce the prevalence of iron-deficiency anaemia (IDA) among adolescent girls and boys
ii. Enable sexual and reproductive health
- Improve knowledge, attitudes and behaviour, in relation to SRH
- Reduce teenage pregnancies
- Improve birth preparedness, complication readiness and provide early parenting support for adolescent parents
iii. Enhance Mental Health
- Address mental health concerns of adolescents
iv. Prevent injuries and violence
- Promote favourable attitudes for preventing injuries and violence (including GBV) among adolescents
v. Prevent substance misuse
- Increase adolescents’ awareness of the adverse effects and consequences of substance misuse
vi. Address conditions for NCDs
- Promote behaviour change in adolescents to prevent NCDs such as cancer, diabetes, cardio-vascular diseases and strokes
3. Rashtriya Bal SwasthyaKaryakram (RBSK)
- Rashtriya Bal SwasthyaKaryakram (RBSK), is a Child Health Screening , a systemic approach of early identification of medical conditions and link to care, support and treatment. This programme subsumes the existing school health programme.
- This program involves screening of children from birth to 18 years of age for 4 Ds- Defects at birth, Diseases, Deficiencies and Development delays, spanning 32 common health conditions for early detection and free treatment and management, including surgeries at tertiary level.
Objective –
Early identification and early intervention for children from birth to 18 years to cover 4 ‘D’s viz.
- Defects at birth,
- Diseases in children,
- Deficiency conditions and
- Developmental delays including Disabilities.
Target group under Child Health Screening and Intervention Service Categories.
| Categories | Age Group |
|---|---|
| Babies born at public health facilities and home – | Birth to 6 weeks |
| Preschool children in rural areas and urban slum | 6weeks to 6 years |
| School children enrolled in class 1st and 12th ingovernment and government aided schools | 6yrs to 18 yrs |
| Selected Health Conditions for Child Health Screening & Early Intervention Services | |
| Defects at Birth 1. Neural tube defect 2. Down’s Syndrome 3. Cleft Lip & Palate / Cleft palate alone 4. Talipes (club foot) 5. Developmental dysplasia of the hip 6. Congenital cataract 7. Congenital deafness 8. Congenital heart diseases 9. Retinopathy of Prematurity | Deficiencies 10. Anemia especially Severe anemia 11. Vitamin A deficiency (Bitot spot) 12. Vitamin D Deficiency, (Rickets) 13. Severe Acute Malnutrition 14. Goiter |
| Diseases of Childhood 15. Skin conditions (Scabies, fungal infection and Eczema) 16. Otitis Media 17. Rheumatic heart disease 18. Reactive airway disease 19.Dental conditions 20. Convulsive disorders | Developmental delays and Disabilities 21. Vision Impairment 22. Hearing Impairment 23. Neuro-motor Impairment 24. Motor delay 25. Cognitive delay 26. Language delay 27. Behavior disorder (Autism) 28. Learning disorder 29. Attention deficit hyperactivity disorder |
| 30. Congenital Hypothyroidism, Sickle cell anemia, Beta thalassemia (Optional) |
Selected Health Conditions for Child Health Screening & Early Intervention Services
Defects at Birth
1. Neural tube defect
2. Down’s Syndrome
3. Cleft Lip & Palate / Cleft palate alone
4. Talipes (club foot)
5. Developmental dysplasia of the hip
6. Congenital cataract
7. Congenital deafness
8. Congenital heart diseases
9. Retinopathy of Prematurity
Deficiencies
10. Anemia especially Severe anemia
11. Vitamin A deficiency (Bitot spot)
12. Vitamin D Deficiency, (Rickets)
13. Severe Acute Malnutrition
14. Goiter
Diseases of Childhood
15. Skin conditions (Scabies, fungal infection and Eczema)
16. Otitis Media
17. Rheumatic heart disease
18. Reactive airway disease
19.Dental conditions
20. Convulsive disorders
Developmental delays and Disabilities
21. Vision Impairment
22. Hearing Impairment
23. Neuro-motor Impairment
24. Motor delay
25. Cognitive delay
26. Language delay
27. Behavior disorder (Autism)
28. Learning disorder
29. Attention deficit hyperactivity disorder
30. Congenital Hypothyroidism, Sickle cell anemia, Beta thalassemia (Optional)
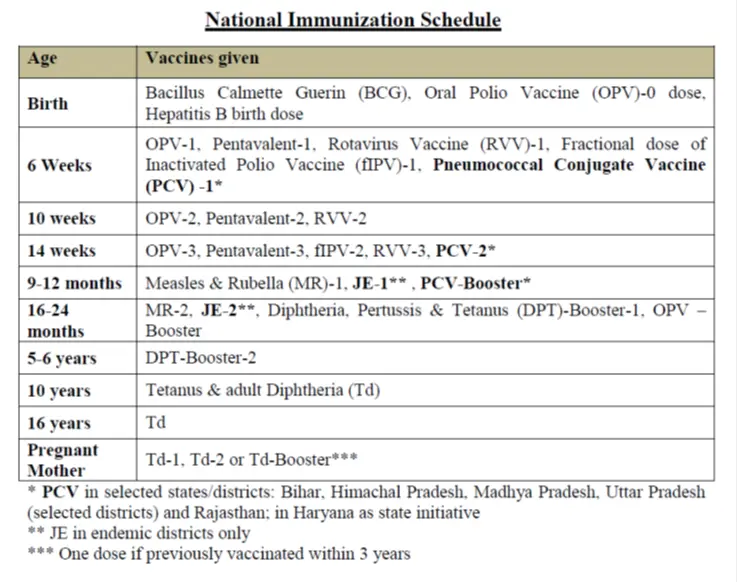
4. Universal Immunisation Programme (UIP)
First Immunization Programme in India was introduced in 1978 as ‘Expanded Programme of Immunization’ (EPI)
In 1985, the programme was modified/renamed as ‘Universal Immunization Programme’ (UIP).
UPI is a one of largest health programme in the world.
Through UIP, MoHFW of India provides several vaccines free of cost to:
- Infants
- Children and
- Pregnant women
Through UIP, Government of India is providing vaccination free of cost against vaccine preventable diseases include diphtheria, pertussis, tetanus, polio, measles, severe form of childhood tuberculosis, hepatitis B, meningitis and pneumonia (Hemophilus influenza type B infections), Japanese encephalitis (JE) in JE endemic districts with introduction of newer vaccines such as rotavirus vaccine, IPV, adult JE vaccine, pneumococcal conjugate vaccine (PCV) and measles-rubella (MR) vaccine in UIP/national immunization programme.
5. Mission Indradhanush / Intensified Misson Indradhanush
Mission Indradhanush programme is launched in December 2014 to achieve full immunization coverage for all children (up to two years of age) and pregnant women at a rapid pace, by the Government of India
Objective of Mission Indradhanush and Intensified Mission Indradhanush (IMI):
To boost the routine immunization coverage/full immunization/100 % Immunization
Goal of Mission Indradhanush:
The ultimate goal of Mission Indradhanush is to ensure full immunization with all available vaccines for children up to two years of age and pregnant women.
Intensified Mission Indradhanush (IMI)
To further intensify the immunization programme,the Intensified Mission Indradhanush (IMI) was launched on October 8, 2017.
The aims of IMI is to reach each and every child up to two years of age and all those pregnant women who have been left uncovered under the routine immunisation programme/UIP.
Intensified Mission Indradhanush has covered low performing areas in the selected districts (high priority districts) and urban areas. Special attention was given to unserved/low coverage pockets in sub-centre and urban slums with migratory population. The focus was also on the urban settlements and cities identified under National Urban Health Mission (NUHM).
Intensified Mission Indradhanush (IMI) 2.0
To boost the routine immunization coverage in the country, Government of India has introduced Intensified Mission Indradhanush 2.0 to ensure reaching the unreached with all available vaccines and accelerate the coverage of children and pregnant women in the identified districts and blocks from December 2019-March 2020.
The IMI 2.0 aims to achieve targets of full immunization coverage in 272 districts in 27 States and at block level (652 blocks) in Uttar Pradesh and Bihar among hard-to-reach and tribal populations.
6. Janani Suraksha Yojana (JSY)
Under the National Rural Health Mission (NRHM), Janani Suraksha Yojana (JSY), is being implemented with the objective of reducing maternal and neo-natal mortality by promoting institutional delivery among the poor pregnant women.
The Yojana, launched on 12th April 2005, by the Hon’ble Prime Minister. JSY is a 100 % centrally sponsored.
Features of JSY
- The scheme focuses on the poor pregnant woman (BPL) for states having low institutional delivery rates namely the states of Uttar Pradesh, Uttaranchal, Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Assam, Rajasthan, Orissa and Jammu and Kashmir. While these states have been named as Low Performing States (LPS), the remaining states have been named as High performing States (HPS).
- Eligibility for Cash Assistance: BPL Certification – This is required in all HPS states.
- Scale of Cash Assistance for Institutional Delivery:
| Category | Rural Area | Total | Urban Area | Total | ||
| Mother’s Package | Asha’s Package | Rs | ||||
| LPS | 1400 | 600 | 2000 | 1000 | 200 | 1200 |
| HPS | 700 | 700 | 600 | 600 |
7. Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA)
Pradhan Mantri SurakshitMatritva Abhiyan (PMSMA) was launched in the year 2016 under National Health Mission. The program aims to provide antenatal care(ANC), free of cost, universally to all pregnant women on the 9th of every month across the country. If the 9th day of the month is a Sunday/ a holiday, then the Clinic is to be organized on the next working day.
Goal of the PMSMA
Pradhan Mantri SurakshitMatritva Abhiyan provides Antenatal Care (ANC) including diagnostics and counselling services as part of the Reproductive Maternal Neonatal Child and Adolescent Health (RMNCH+A) Strategy.
Objectives of the program:
- Ensure at least one antenatal checkup for all pregnant women in their second or third trimester by a physician/specialist
- Improve the quality of care during ante-natal visits. This includes ensuring provision of the following services:
- All applicable diagnostic services
- Screening for the applicable clinical conditions
- Appropriate management of any existing clinical condition such as Anaemia, Pregnancy induced hypertension, Gestational Diabetes etc.
- Appropriate counselling services and proper documentation of services rendered
- Identification of high risk pregnancies based on obstetric/ medical history and existing clinical conditions.
- Appropriate birth planning for each pregnant woman especially those identified with any risk factor or comorbid condition.
- Special emphasis on early diagnosis, adequate and appropriate management of women with malnutrition.
Every pregnancy is special and every pregnant woman must receive special care’. Any pregnant woman can develop life-threatening complications with little or no advance warning, so all pregnant women need access to quality antenatal services to detect and prevent life-threatening complications during childbirth.
8. Navjaat Shishu Suraksha Karyakram (NSSK)
It is a training programme of health care personals.
NSSK is a programme aimed to train health personnel in basic newborn care and resuscitation (care at birth issues i.e. Prevention of Hypothermia, Prevention of Infection, Early initiation of Breast feeding and Basic Newborn Resuscitation).
Objective
Objective is to have a trained health personal in basic newborn care and resuscitation at every delivery point. The training is for 2 days and is expected to reduce neonatal mortality significantly in the country.
9. National Programme for Family planning
India was the first country in the world to have launched a National Programme for Family Planning in 1952.
Currently NPFP promotes population stabilization goals as well as promotes reproductive health and reduce maternal, infant & child mortality and morbidity.
Under the programme public health sector provides various family planning services at various levels of health system.
Mission Pariwar Vikas
MoHFW launched “Mission Pariwar Vikas”in 2016 with an aim to ensure availability of contraceptive methods at all the levels of Health Systems.
Goal –
Its overall goal is to reduce India’s overall fertility rate to 2.1 by the year 2025
Objective –
Improving access to contraceptives through delivering assured services, ensuring commodity security and accelerating access to high quality family planning services.
Key strategies include –
- Providing more choices through newly introduced contraceptives: Injectable Contraceptive, MPA (Medroxyprogesterone acetate) under Antara program and Chaya (earlier marketed as Saheli) will be made freely available to all government hospitals.
- Emphasis on Spacing methods like IUCD
- Revitalizing Postpartum Family Planning including PPIUCD in order to capitalize on the opportunity provided by increased institutional deliveries. Appointment of counsellors at high institutional delivery facilities is a key activity.
- Strengthening community-based distribution of contraceptives by involving ASHAs and Focused IEC/ BCC efforts for enhancing demand and creating awareness on family planning
- Availability of Fixed Day Static Services at all facilities.
- Emphasis on minilap tubectomy services because of its logistical simplicity and requirement of only MBBS doctors and not post graduate gynecologists/ surgeons.
- A rational human resource development plan for IUCD, minilap and NSV be chalked up to empower the facilities (DH, CHC, PHC, SHC) with at least one provider each for each of the services and Sub Center’s with ANMs trained in IUD insertion
- Ensuring quality care in Family Planning services by establishing Quality Assurance Committees at state and district levels Plan for accreditation of more private/ NGO facilities to increase the provider base for family planning services under PPP.
- Increasing male participation and promoting Non-scalpel vasectomy.
- Demand generation activities in the form of display of posters, billboards and other audio and video materials in the various facilities be planned and budgeted.
- Strong Political Will and Advocacy at the highest level, especially in states with high fertility rates.
Hum Do
The National Family Planning Programme, through Hum Do aims to provide eligible couples with information and guidance on family planning methods and services available, to ensure individuals and couples lead a healthy, happy and prosperous life.
II. NATIONAL NUTRITIONAL PROGRAMMES
- National Iodine Deficiency Disorders Control Programme
- MAA (Mothers’ Absolute Affection) Programme for Infant and Young Child Feeding
- National Programme for Prevention and Control of Fluorosis (NPPCF)
- National Iron Plus Initiative for Anaemia Control
- National Vitamin A prophylaxis Programe
- Integrated Child Development Services (ICDS)
- Mid-Day Meal Programme
1. National Iodine Deficiency Disorders Control Programe
In 1992, the National Goiter Control Programme (NGCP) was renamed as National Iodine Deficiency Disorder Control Programme (NIDDCP).
Iodine is a micronutrient and normally required around 100-150 microgram for normal growth and developmenre. It is also quired for the synthesis of the thyroid hormones, thyroxine (T4) and triiodothyronine (T3) and essential for the normal growth and development and well being of all humans.
Deficiency of iodine may cause following disorders:
- Goiter
- Subnormal intelligence
- Neuromuscular weakness
- Endemic cretinism
- Still birth
- Hypothyroidism
- Defect in vision, hearing, and speech
- Spasticity
- Intrauterine death
- Mental retardation
Objectives:
- Surveys to assess the magnitude of the Iodine Deficiency Disorders.
- Supply of iodated salt in place of common salt.
- Resurvey after every 5 years to assess the extent of Iodine Deficiency Disorders and the impact of lodated salt.
- Laboratory monitoring of iodated salt and urinary iodine excretion.
- Health education and Publicity.
2. MAA-(Mothers’ Absolute Affection) Programme for Infant and Young Child Feeding
MAA – “Mother’s Absolute Affection” is a nationwide programme on promotion of breastfeeding and provision of counselling services for supporting breastfeeding to lactating mother through health systems/health care professionals.
Goal
- Promotion, protection and support of breastfeeding practices through health systems to achieve higher breastfeeding rates.
Objective
- awareness generation activities for breastfeeding targeting pregnant and lactating (positioned as an important intervention for child survival and development during feeding).
- Processes in place for lactation management.
Key components of the programme are –
- Communication for enhanced awareness and demand generation through mass media and mid media;
- Training and capacity enhancement of nurses at government institutions, and all ANMs and ASHAs. They will provide information and counselling support to mothers for breastfeeding;
Key messages –
- Early initiation of breastfeeding; immediately after birth, preferably within one hour.
- Breast-milk alone is the best food and drink for an infant for the first six months of life. No other food or drink, not even water, is usually needed during this period. But allow infant to receive ORS, drops, syrups of vitamins, minerals and medicines when required for medical reasons.
- After 6 months of age, babies should be introduced to semi-solid, soft food (complementary feeding) but breastfeeding should continue for up to two years and beyond.
During an illness, children need additional fluids and encouragement to eat regular meals, and breastfeeding infants need to breastfeed more often. After an illness, children need to be offered more food than usual, to replenish the energy and nourishment lost due to the illness.
3. National Programme for Prevention and Control of Fluorosis (NPPCF)
Fluorosis is caused by excess intake of fluoride through drinking water/food products/industrial emission over a long period. It results in major health disorders like dental fluorosis, skeletal fluorosis and non-skeletal fluorosis.
Goal
- The NPPCF aims to prevent and control Fluorosis cases in the country.
Objectives
- Assess and use survey data of fluorosis of Ministry of Drinking water & Sanitation;
- Capacity building for prevention, diagnosis and management of fluorosis cases in the selected/affected area.
4. National Iron Plus Initiative for Anaemia Control
- National Iron+ Initiative was launched by the Adolescent Division of the Ministry of Health andFamily Welfare (MoHFW), Government of India.
- Anemia is more vulnerable groups such as pregnant women, infants, young children and adolescents.
- Iron deficiency being the most common form nutritional anemia.
Aim
- To reach the following age groups for supplementation of Iron & Folic Acid
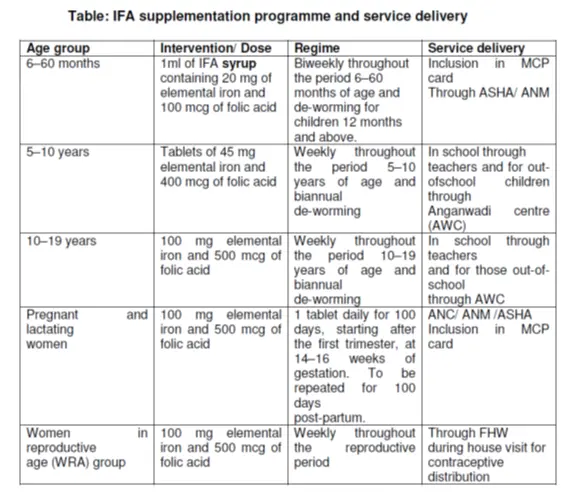
WEEKLY IRON FOLIC ACID SUPPLEMENTATION (WIFS)
1. Objective
Objective of Weekly Iron Folic acid Supplementation (WIFS) To reduce the prevalence and severity of anaemia in adolescent population (10-19 years).
ii. Target groups
- School going adolescent girls and boys in 6th to 12th class enrolled in government/government aided/municipal schools.
- Out of school adolescent girls (10-19 years).
iii. Intervention
- Administration of Weekly Iron-folic Acid Supplements of 100mg elemental iron and 500ug Folic acid using a fixed day approach.
5. National Vitamin ‘A’ prophylaxis Program
Vitamin A is an important micronutrient for maintaining normal growth, regulatingcellular proliferation and differentiation, controlling development, and maintainingvisual and reproductive functions.
Prevalence of clinical and sub clinical vitamin A deficiency in India is among the highest in the world.
Aim: to decrease the prevalence of Vitamin A deficiency
Prophylactic Vitamin A as per the following dosage schedule:
- 100000 IU at 9 months with measles immunization
- 200000 IU at 16-18 months, with DPT booster
- 200000 IU every 6 months, up to the age of 5 years.
Thus, a total of 9 mega doses are to be given from 9 months of age up to 5 years.
6. Integrated Child Development Services (ICDS)
Integrated Child Development Service (ICDS) scheme was launched on 2nd October, 1975.
Beneficiaries:
- Children below 6 years
- Pregnant and lactating women
- Women in the age group of 15-44 years
- Adolescent girls in selected blocks
Objectives:
- Improve the nutrition and health status of children in the age group of 0-6 years
- Lay the foundation for proper psychological, physical and social development of the child
III. COMMUNICABLE DISEASES
1. Integrated Disease Surveillance Programme (IDSP)
The Integrated Disease Surveillance Program (IDSP) was initiated in assistance with World bank, in the year 2004.
The scheme aimed to strengthen disease surveillance for infectious diseases to detect and respond to outbreaks immediately. The Central Surveillance Unit (CSU) at the National Centre for Disease Control (NCDC), receives disease outbreak reports from the States/UTs on weekly basis.
State/District Surveillance Units analyses this data weekly, to interpret the disease trends and seasonality of diseases.
The surveillance data is collected on three specified reporting formats- SPL
- “S”-(suspected cases
- “P” -presumptive cases
- “L”- laboratory confirmed cases
3. National Tuberculosis Elimination Programme
The National TB Programme (NTP) was launched by the Government of India in 1962 I (Include both BCG vaccination and TB treatment). In 1978, BCG vaccination was shifted under the Expanded Programme on Immunisation & Now comes Under UIP.
In 1993, the WHO declared TB as a global emergency, adevised the directly observed treatment – short course (DOTS), and recommended to follow it by all countries.
After that NTP as Revised National TB Control Programme (RNTCP) in the e year 1993.
DOTS was officially launched as the RNTCP strategy in 1997.
National strategic plan for tuberculosis elimination 2017-2025’-
RNTCP has released a ‘National strategic plan for tuberculosis 2017-2025’ (NSP) for the control and elimination of TB in India by 2025. According to the NSP TB elimination have been integrated into the four strategic pillars of DTPB
- Detect
- Treat
- Prevent
- Build
1) Detect:
The first objective of NSP is to detect all drug sensitive TB cases (DS-TB) and drug resistant TB cases (DRTB).
Notification of TB cases: Notification of all TB patients from all health care providers (Both Govt & Private secors) is made mandatory since 2012. With its amendment in 2015, all laboratories are also included to notify TB cases.
NIKSHAY: It is a web-based TB surveillance system called “NIKSHAY” (https://nikshay.gov.in ) for both government and private health care facilities.
Private providers are provided incentives for TB case notification, through direct beneficiary transfer to facilitate.
The incentives to the Private Sector TB Care Provider are as follows:
- Rs 250/- on notification of a TB case diagnosed as per Standards for TB Care in India (STCI)
- Rs 250/- on completion of every month of treatment
- Rs 500/- on completion of entire course of TB treatment
- Rs 2750/ for notification and management of a drug-sensitive patient over 6-9 months as per STCI
- Rs 6750/-for notification and correct management of a drug-resistant case over 24 months as per STCI
Free drugs and diagnostic tests to TB patients in private sector- Free drugs and diagnostic tests are provided to TB patients seeking treatment from private health sector.
2) Treat:
ALL TB patients must get appropriate Anti-TB treatment under directly observed treatment DOT.
DOT is a specific strategy, to improve adherence by any person observing the patient taking medications in real time. The treatment observer does not need to be a health-care worker, but could be a friend, a relative or a lay person who works as a treatment supervisor or supporter. If treatment is incomplete, patients may not be cured and drug resistance may develop).
Treatment Strategy of TB
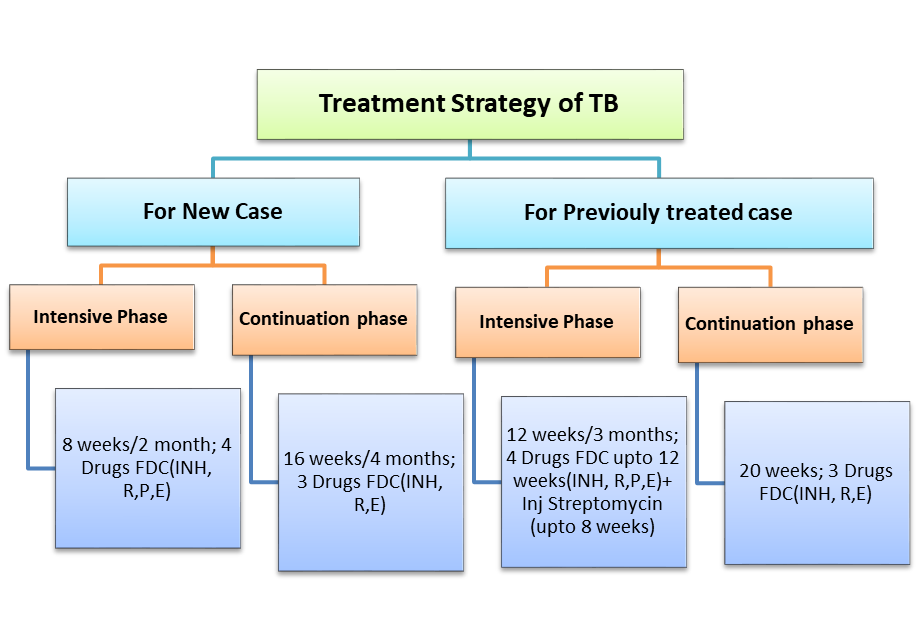
The continuation phase in both new and previously treated cases may be extended by 12-24 weeks in certain forms of TB like skeletal, disseminated TB based on clinical decision of the treating physician.
RNTCP has introduced new drug Bedaquiline CAP for MDR-TB under conditional access programme in 2016. (Pharmacist GSSSB 2020)
Nikshya poshak yozana: Unnder National Health Mission (NHM), financial incentive of Rs.500/- per month is provided for nutritional support to each notified TB patient for duration for which the patient is on anti-TB treatment through Direct benefit transfer (DBT).
Expending options for ICT based treatment adherence support mechanisms:
- Mobile based “Pill-in-Hand” adherence monitoring tool
- Interactive Voice Response (IVR), SMS reminders.
- Specially designed electronic pill boxes or strips with GSM connection and pressure sensor
- Patient Compliance toolkit: a mobile app for patients to report treatment compliance using video, audio or text message
- Automated pill loading system
- innovatively designed ICT enabled smart cards SMS gateway
Intensifying TB control activities in following key populations is addressed in NSP:
- TB-HIV
- Diabetics, Tobacco use and Alcohol dependence
- Poor, undernourished, economically and socially backward communities
- TB control in hilly and difficult terrains
- Substance dependence and sexual minorities
- TB and pregnancy
- Paediatric population
- Prison Inmates and staff of prisons/jails
- management of extra pulmonary TB
3) Prevent:
With the objective to prevent emergence of TB in susceptible population various measures are indicated as:
- Scale up air-borne infection control measures at health care facilities
- Treatment for latent TB infection in contacts of bacteriologically-confirmed cases
TB can be Prevent by following
a) Air borne infection control measures– by controlling Air borne infection useful to minimizing the risk of TB transmission within population and hospital
b) Contact tracing-Since transmission can occur from case to the contact any time (before diagnosis or during treatment) all contacts of TB patients must be evaluated. T
c) Isoniazid Preventive Therapy (IPT)–
Preventive therapy is recommended to Children < 6 years of age, who are close contacts of a TB patient.
In addition to above, INH preventive therapy will be considered in following situation:
- For all HIV infected children who either had a known exposure to an infectious TB case or are Tuberculin skin test (TST) positive (>=5mm induration) but have no active TB disease.
- All Tuberculin skin test (TST) positive (>=5mm induration) positive children
- A child born to mother who was diagnosed to have TB in pregnancy will receive prophylaxis for 6 months, provided congenital TB has been ruled out. BCG vaccination can be given at birth even if INH preventive therapy is planned.
d) BCG vaccination– It is provided at birth or as early as possible till one year of age.
e) Addressing social determinants of TB like poverty, malnutrition, urbanization, indoor air pollution, etc. require inter departmental/ ministerial coordinated activities and the programme is proactively facilitating this coordination.
4. Build:
Health system strengthening for TB control under the National Strategic Plan 2017-2025 is recommended in the form of building and strengthening enabling policies, empowering institutions and human resources with enhanced capacities.
4. National Leprosy Eradication Programme (NLEP)
National Leprosy Control Programme (NLCP) was launched by the Govt. of India in 1954- 55.
National Leprosy Eradication Programme was introduced in 1983.
Leprosy is caused by a bacterium called Mycobacterium leprae which spreads from an untreated case of multi-bacillary leprosy (severe form) to others through drop-let (air-borne) whenever a person with multi-bacillary leprosy coughs are sneezes.
OBJECTIVE
- Elimination of leprosy i.e. prevalence of less than 1 case per 10,000 population in all districts of the country.
- Strengthen Disability Prevention & Medical Rehabilitation of persons affected by leprosy.
5. National Centre for Vector Borne Diseases Control
National Vector Borne Disease Control Programme (NVBDCP) is tthe agency for prevention and control of six vector borne diseases (VBDs) i.e. Malaria, Dengue, Lymphatic Filariasis, Kala-azar, Japanese Encephalitis and Chikungunya in India. Out of six diseases, three disease namely Malaria, Lymphatic Filariasis & are targeted for elimination.
NCVBD programme was Launched in 2002 by merging National anti -malaria control programme , National Filaria Control Programme and Kala Azar Control programmes . After that Japanese B Encephalitis and Dengue/DHF have also been included in this Program.
List of Vector Borne Diseases Control Programme Legislations:
1) National Anti – Malaria programme
2) Kala – Azar Control Programme
3) National Filaria Control Programme
4) Japenese Encephilitis Control Programme
5) Dengue and Dengue Hemorrhagic fever
6) chikungunya
1) NATIONAL ANTI – MALARIA PROGRAMME
In April 1953, Govt. of India launched a National Malaria Control Programme (NMCP).
National Malaria Eradication Programme (NMEP) -1958
EMCP (Enhanced Malaria Control Programme) with World Bank-1997
IMCP (Intensified Malaria Control Project)-2005
Objective:
- To bring down malaria transmission to a level at which it would cease to be a major public health problem.
2) KALA -AZAR CONTROL PROGRAMME
Kala-azar or visceral leishmaniasis (VL) is a chronic disease caused by an intracellular protozoan (Leishmania species) and transmitted to man by bite of female phlebotomus sand fly.
Objectives:
The strategy for kala-azar control broadly included three main activities.
- Interruption of transmission by reducing vector population through indoor residual insecticides.
- Early diagnosis and complete treatment of Kala-azar cases; and
- Health education programme for community awareness.
3) NATIONAL FILARIA CONTROL PROGRAMME
The National Filaria Control Programme was launched in 1955.
Bancroftian filariasis caused by Wuchereria bancrofti, which is transmitted to man by the bites of infected mosquitoes – Culex, Anopheles, Mansonia and Aedes.
Brugian filariasis caused by Brugia malayi
Objectives:
- Reduction of the problem in un-surveyed areas
- Control in urban areas through recurrent anti-larval and anti-parasitic measures.
4) JAPANESE ENCEPHALITIS CONTROL PROGRAMME
Japanese encephalitis (JE)/दिमागी बुखार is a zoonotic disease and caused by an arbovirus, group B (Flavivirus) and transmitted by Culex mosquitoes.
Directorate of National Anti-Malaria Programme is monitoring JE situation in the country.
Objectives:
- Strengthening early diagnosis and prompt case management through training of medical and nursing staff.
- Vector control measures mainly fogging during outbreaks, space spraying in animal dwellings, and antilarval operation where feasible; and
- Development of a safe and standard indigenous vaccine. Vaccination for high risk population particularly children below 15 years of age.
5) DENGUE AND DENGUE HEMORRHAGIC FEVER
One of the most important resurgent tropical infectious disease is dengue.
Dengue Fever and Dengue Hemorrhagic Fever (DHF) are acute fevers caused by four dengue virus serotypes (DEN 1,2,3 and 4) transmitted by the infected mosquitoes, Aedes aegypti.
The Vector Aedes Aegypti breed in peridomestic fresh water collections.
Objectives:
- Surveillance for disease and outbreaks
- Early diagnosis and prompt case management
- Vector control through community participation and social mobilization
6) Chikugunya
- Chikungunya, also called chikungunya virus disease or chikungunya fever, is a viral illness that is spread by the bite of infected mosquitoes.
- The disease resembles dengue fever, and is characterized by severe, sometimes persistent, joint pain (arthiritis), as well as fever and rash.
- There is no specific treatment for chikungunya.
- Prevention centers on avoiding mosquito bites in areas where chikungunya virus may be present, and by eliminating mosquito breeding sites.
6. Programme for Prevention and Control of leptospirosis
Leptospirosis is a zoonotic disease caused by Leptospira bacteria found in urine of rodents, cattle, pigs etc.
Objective of the Programme is to reduce the morbidity and mortality due to leptospirosis in Humans.
7. National AIDS Control Programme (NACP)
- The National AIDS Control Programme (NACP), launched in 1992, a programme for prevention and control of HIV/AIDS in India.
- Objective : slowing down the spread of HIV infections so as to reduce morbidity, mortality and impact of AIDS in the country.
- In November 1999, the second National AIDS Control Project (NACP II) was launched with World Bank with two key objective-
- to reduce the spread of HIV infection in India, and
- to increase India’s capacity to respond to HIV/AIDS on a long-term basis
| Phase | Launching Year | Objective & Goals |
| NACP Ist | 1992 | slowing down the spread of HIV infections |
| NACP IIst | 1999 | to reduce the spread of HIV infection in India, and to increase India’s capacity to respond to HIV/AIDS on a long-term basis |
| NACP IIIst | 2007 | halting and reversing the HIV epidemic in India over its five-year period by scaling up prevention efforts among High Risk Groups (HRG) and General Population and integrating them with Care, Support & Treatment services |
| NACP IVst | Reduce new infections by 50% (2007 Baseline of NACP III) Comprehensive care, support and treatment to all persons living with HIV/AIDS | |
| NACP Vst | ending the HIV/AIDS epidemic as a public health threat by 2030 through a comprehensive package of prevention, detection and treatment services.by using HIV/AIDS Prevention and Control Act (2017), |
The Phase V builds upon the by using HIV/AIDS Prevention and Control Act (2017), ending the HIV/AIDS epidemic as a public health threat by 2030 through a comprehensive package of prevention, detection and treatment services.
The HIV & AIDS (P & C) Act, 2017
The HIV and AIDS (Prevention & Control) Act, 2017 is a central legislation protecting and promoting the rights of persons infected with and affected by HIV and AIDS. The Act came into force on September 10, 2018 with the objective to prevent and control the spread of HIV and AIDS and for reinforcing the legal and human rights of persons infected with and affected by HIV and AIDS. It also seeks to protect the rights of healthcare providers.
The Act addresses stigma & discrimination and strives to create an enabling environment for enhancing access to services. It provides for diagnostic facilities related to ART and opportunistic infection management to people living with HIV and AIDS.
8. Pulse Polio Programme
- Pulse Polio Immunization programme was launched in India in 1995.
- Children in the age group of 0-5 years administered polio drops during National and Sub-national immunization rounds (in high risk areas) every year.
- The last polio case in the country was reported from Howrah district of West Bengal with date of onset 13th January 2011. Thereafter no polio case has been reported in the country (25th May 2012).
- WHO on 24th February 2012 removed India from the list of countries with active endemic wild polio virus transmission.
Objective :
The Pulse Polio Initiative was started with an objective of achieving hundred per cent coverage under Oral Polio Vaccine.
National Immunization Day (NID) commonly known as Pulse Polio Immunization programme was launched in India in 1995, and is conducted twice in early part of each year. Additionally multiple rounds (at least two) of sub national immunization day (SNID) have been conducted over the years in high risk states/areas. In these campaigns, children in the age group of 0-5 years are administered polio drops.
1. South-East Asia Region of WHO including India has been certified polio free by “The Regional Certification Commission (RCC)” on 27th March 2014.
2. India reported its last polio case from district Howrah, West Bengal on 13th January, 2011.
3. WHO on 24th February 2012 removed India from the list of “endemic countries with active polio virus transmission”
Steps taken by the Government to maintain polio free status in India
- Maintaining community immunity through high quality National and Sub National polio rounds each year.
- An extremely high level of vigilance through surveillance across the country for any importation or circulation of poliovirus and VDPV is being maintained. Environmental surveillance (sewage sampling) have been established to detect poliovirus transmission and as a surrogate indicator of the progress as well for any programmatic interventions strategically in Mumbai, Delhi, Patna, Kolkata Punjab and Gujarat.
- All States and Union Territories in the country have developed a Rapid Response Team (RRT) to respond to any polio outbreak in the country. An Emergency Preparedness and Response Plan (EPRP) has also been developed by all States indicating steps to be undertaken in case of detection of a polio case.
- To reduce risk of importation from neighbouring countries, international border vaccination is being provided through continuous vaccination teams (CVT) to all eligible children round the clock. These are provided through special booths set up at the international borders that India shares with Pakistan, Bangladesh, Bhutan Nepal and Myanmar.
- Government of India has issued guidelines for mandatory requirement of polio vaccination to all international travelers before their departure from India to polio affected countries namely: Afghanistan, Nigeria, Pakistan, Ethiopia, Kenya, Somalia, Syria and Cameroon. The mandatory requirement is effective for travellers from 1st March 2014.
- A rolling emergency stock of OPV is being maintained to respond to detection/importation of wild poliovirus (WPV) or emergence of circulating vaccine derived poliovirus (cVDPV).
- National Technical Advisory Group on Immunization (NTAGI) has recommended Injectable Polio Vaccine (IPV) introduction as an additional dose along with 3rd dose of DPT in the entire country in the last quarter of 2015 as a part of polio endgame strategy.
National Viral Hepatitis Control Program
National Programme on Containment of Anti-Microbial Resistance
National Rabies Control Program
Join WhatsApp channel to get latest Job notification, Study material, Previous paper, MCQ quiz, Admission alerts & News etc. for Pharmacy aspirants.
Subscribe our Telegram channel for Pharmacy Notes, MCQ Quiz, , Previous paper, Admission alerts & News etc. for Pharmacy professionals.
Join Telegram group for all Pharmacy books, Pharmacopoeia (IP, USP, BP), Pharmacy Notes, Previous Year Question papers in pdf format.







